Study of Serum Uric Acid Levels in Patients with Type 2 Diabetes Mellitus and its Association with Cardiac Risks Factors and Complications
Shivakumar BG1, Krishnamurthy KH2, Kiran Kumar BN3, Ajeya Kashyap CA4 , Kunal Jhaveri5
Associate Professor, Department of General Medicine, JJM Medical College, Davangere, Karnataka, India.
Lead Medical Advisor, Global Medical Affairs, Dr Reddy’s Laboratories, Hyderabad, Telangana, India.
Senior Resident, KMC Manipal, Manipal, Karnataka, India.
Post-graduate, JJM Medical College, Davangere, Karnataka, India.
DGM - Medical Services, Zydus Healthcare Limited, Goregaon East, Mumbai, Maharashtra, India.
Corresponding Author: Shivakumar BG, Associate Professor, Department of General Medicine, JJM Medical College, Davangere, Karnataka, India.
Email: shivu0033@gmail.com
Article information
Received date: 19/07/2020; Accepted date: 18/02/2021; Published date: 01/03/2021
Introduction
Introduction: The prevalence of diabetes mellitus (DM) is rapidly rising all over the world. India is called the capital of the diabetic world. DM is an important risk factor for cardiovascular disease (CVD). Many studies have shown that serum uric acid concentration can predict the risk of cardiac complications.
Aim: This study was conducted to assess the direct or indirect effect of serum uric acid on cardiovascular risk and complications.
Methods: 80 patients with type 2 DM aged >40 years meeting the criteria for diagnosing Type 2 DM as per the American Diabetic Association (ADA) were recruited in the study. Patients with renal failure and type 1 DM were excluded. Patients were further subjected to investigations like serum uric acid, electrocardiogram (ECG), two- dimensional echocardiogram (2D echo) and other routine investigations. Urine albumin levels, troponin I, chest X-rayand ultrasonography (USG) abdomen were done. Investigation reports were analyzed with the clinical profile and the data was compiled and an appropriate statistical test was applied.
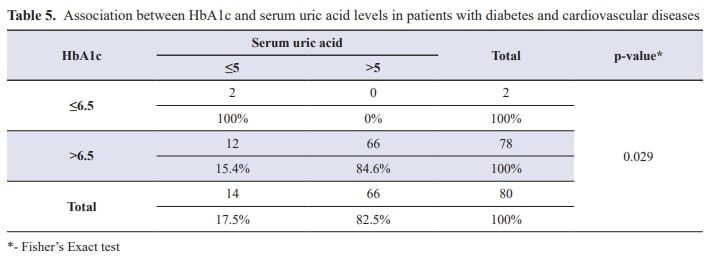
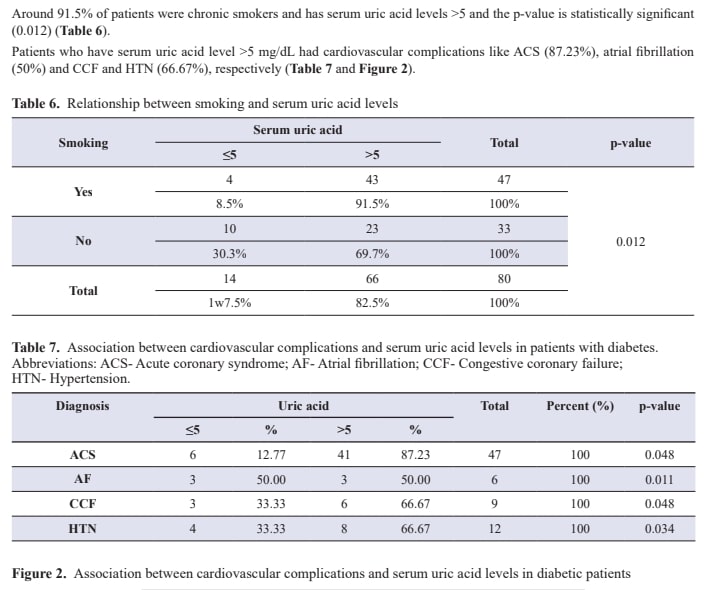
Results: In this study, serum uric acid levels were measured in patients with type 2 DM and were found out to have a significant correlation with the cardiovascular risk factor. About 82.5% of the diabetic patients with cardiovascular disease had serum uric acid levels >5 mg/dL. 66.67% of the known type 2 DM with hypertension have serum uric acid levels >5 mg/dL. 96.9% of the patients had a body mass index (BMI) more than the normal range, i.e., >23 kg/m2. 91% of the patients who were chronic smokers had serum uric acid levels >5 mg/dL. It was observed that among cardiovascular complications, 87.23% of the acute coronary syndrome (ACS) patients, 50% of the patients with atrial fibrillation, 66.67% of the patients with congestive cardiac failure (CCF) and hypertension (HTN) patients had serum uric acid levels >5 mg/dL.
Conclusion: Although there is overwhelming evidence that elevated serum uric acid concentrations are strongly associated with increased cardiovascular risks and poor outcomes, prospective population studies are often confounded by coexistent risk factors. In the present study, serum uric acid was correlated with cardiovascular risk factors like obesity (high BMI), hypertension, dyslipidaemia, smoking, and cardiovascular complications like acute coronary syndrome (ACS), congestive heart failure (CCF) and arrhythmias, and these results were statistically significant.
Keywords: Serum uric acid, diabetes, cardiovascular, myocardial infarction
Introduction
Diabetes mellitus is the most common metabolic disorder due to lack of insulin secretion or decreased action or both resulting in an increased glucose level (hyperglycaemia). The prevalence of diabetes is rapidly rising all over the world.1 In the 21st century, diabetes has emerged as one of the major health issues affecting more and more people each year, which results in more complications. Currently, half a billion people are living with diabetes worldwide causing a high risk of CVD.22 Furthermore, around 318 million adults have impaired glucose tolerance and are at risk of developing diabetes in the future.3
India being the diabetic capital of the world,4 population-based studies showing the prevalence of type 2 diabetes in different parts of India has been recently reviewed and showed that the prevalence has risen five-fold, from 2.1% in 1975 to 12.1% in 2000.5 Presently as per 2015 estimation, around India, 69.2 million people have diabetes in India which is estimated to rise to 123.5 million by 2040 which is second to China. Rapid urbanization and industrialization have produced advancement on the social and economic front in developing countries such as India which have resulted in dramatic lifestyle changes leading to lifestyle-related diseases.
Early diagnosis and treatment not only delay the onset of complications6 but also, more importantly, indicate that the onset of diabetes can be prevented or delayed by lifestyle interventions among those identified to be at risk for developing diabetes.7,8 The major complications of diabetes are cardiovascular diseases. Diabetes is associated with a marked increase by a factor of two to four times increased risk of coronary artery disease.9
Since 1950, many epidemiological studies have shown the positive association between serum uric acid level and cardiovascular diseases like ischemic heart disease (IHD) and stroke.10
However, it is still debatable whether uric acid is an independent risk factor for cardiovascular mortality as several studies reported that hyperuricemia is merely associated with cardiovascular disease.11
In recent years, a new debate started about the association between cardiovascular disease and increased serum uric acid levels. Several large studies have shown that the concentration of serum uric acid levels could predict the risk of cardiovascular events like myocardial infarction. The potential mechanism by which uric acid may have a direct or indirect effect on cardiovascular risk has been directed towards research.12
The aims and objectives of our study are to study-
- Serum uric acid levels in type 2 diabetes mellitus.
- The correlation between serum uric acid levels.
- Cardiac risk factors and the correlation between serum uric acid levels and cardiac complications.
Material and Methods
Patients with type 2 diabetes mellitus attending OPD and admitted to the department of medicine of Bapuji Hospital and Chigateri General Hospital, Davangere, Karnataka, India from November 2016 to October 2018 were taken into study.The study protocol was reviewed and approved by the institutional research ethics committee of JJM Medical College, Davangere, Karnataka, India. Patients with type 2 diabetes mellitus, with age >40 years and both sexes were included in the study. Patients with renal failure, renal transplant, and hepatic failure and type 1 diabetes mellitus were excluded from the study. Patients were subjected to investigations like serum uric acid, ECG, 2D echo and other routine investigations. Urine albumin levels, Troponin I, chest x-ray and USG abdomen were done. All blood samples were drawn with the participant in the seated position after a 10-h overnight fast. The serum uric acid was measured by using the uricase peroxidase method.
Results
A total of 80 patients with age group of 40-75 years were included for the study as per the inclusion criteria. Most patients were in the age group of 61-70 years followed by age group of 51-60 years. It is observed that cardiovascular complications in diabetes are maximum between age group of 50-70 years. The study group included 53 males (66%) and 27 females (33.8%), with male preponderance (Table 1).
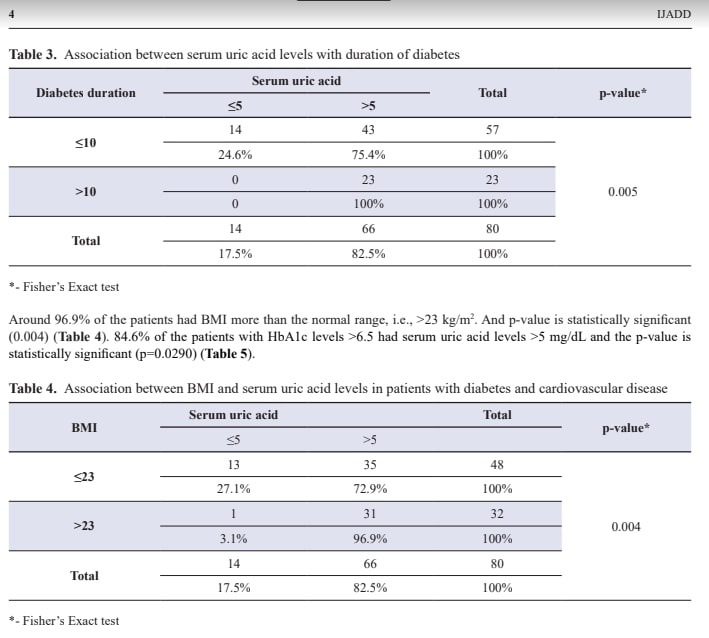
Majority of the patients (82.5%) are diabetes with cardiovascular disease having serum uric acid levels >5 mg/dL and 17.5% patients had < 5 mg/dL (Table 2 and Figure 1). The patients who had longer duration of diabetes (>10 years) had serumuric acid levels >5 mg/dL (p=0.005)
(Table 3).



Discussion
Uric acid, the product of purine metabolism either exogenous or endogenous purines are degraded primarily in the liver and intestine. Uric acid may cause insulin resistance in the liver by inducing oxidative stress and also blocks the vasodilatation ability of the insulin, which is important for the delivery of glucose to skeletal muscle. Less production of adiponectin and inflammation in the adipose tissue is caused by uric acid. Studies show increased levels of uric acid in patients with insulin resistance which could be due to hyperinsulinemia which lowers the uric acid excretion.13 High level of serum uric acid is associated with metabolic syndrome. Association between the elevation of serum uric acid and increased cardiovascular risk was identified for many years.11 Observational studies showed that serum uric acid levels are higher in patients with diabetes with established cardiovascular disease. Studies also showed increased serum uric acid levels cause endothelial dysfunction and increase plasma renin activity.14 However, increased serum uric acid levels are also associated with possible risk factorsc like increased BMI, HTN, and smoking, etc.
Duration of diabetes was positively correlated with uric acid levels. Uric acid levels increase with increasing duration of diabetes and the association was statistically significant. A study conducted by Yoo et al. (2005) and Becker and Jolly etal. (2006) has shown that hyperglycaemia was a remarkable risk factor for hyperuricemia. Another study conducted in Japan involving 3681 patients showed that elevation of serum uric acid concentration in males increased the risk of type 2 diabetes. The conclusion of these studies showed increased serum uric acid was positively associated with hyperglycaemia.15
Sumino et al. (1999) conducted a study to compare uric acid levels in males and females, which showed males had high levels of uric acid compared to females. It may be due to oestrogen that promotes uric acid excretion in females. In the present study, BMI was correlated with serum uric acid levels.16 96.9% of the patients had BMI more than the normal range, i.e., >23kg/m2 and the p-value was statistically significant (0.004).
Another study conducted by Bedir et al. has shown the role of leptin in the regulation of serum uric acid level in humans. This study also shows leptin may be a possible candidate for the missing link between obesity and hyperuricemia.13
Serum uric acid levels are significantly elevated in patients with hypertension.17,18 In this study, 83.3% of the known hypertensive patients have serum uric acid levels >5 mg/dL. A study conducted by Lin KC et al. showed blood pressure levels predict cardiovascular disease incidence synergistically with serum uric acid levels.19 Rat model study demonstrated that uricacid might have a pathogenic role in the development of hypertension, vascular disease and renal disease.20
The serum uric acid levels were significantly higher in diabetic patients with cardiovascular complications. It was observed that among cardiovascular complications, 87.23% of the ACS patients, 50% of the patients with atrial fibrillation, 66.67% of the patients with CCF and HTN patients had serum uric acid levels >5 mg/dL. So, serum uric acid >5 mg/dL should be considered as a red flag in those patients at risk for cardiovascular disease..21,22,15,16
Finland cohort population study had shown the positive association between increased serum uric acid level and obesity,impaired glucose tolerance and hypertension in patients between the age group of 40 to 69 years.13
There are enormous studies that showed that elevated serum uric acid levels are strongly associated with increased risk of cardiovascular risk and a poor outcome. However, some prospective studies are often confounded by co-existence risk factors.11 In the present study, serum uric acid was positively correlated with duration of diabetes, and cardiovascular risk factors like obesity (high BMI, abnormal waist-hip ratio), hypertension and dyslipidaemia and the results were statistically significant. However, studies also showed that decreasing serum uric acid levels doesn’t reduce the risk of cardio-metabolic conditions.23
Limitation of the study
This study has some limitations. It was a cross-sectional design, which limited our ability to assess causal relationships. We did not estimate leptin levels, C peptide levels and plasma insulin levels. The sample size is very small which may have led to bias. We did not estimate serum uric acid excretion and urate clearance. Information about medications, including angiotensin receptor blocker (ARBs), angiotensin-converting enzyme (ACE) inhibitors, diuretics, and urate-lowering agents were not available.
Conclusion
From this study, we can conclude that serum uric acid level was significantly elevated in patients with diabetes, and it was independent of age. Mean serum uric acid levels of male patients were more than that of females. A significant positive correlation was observed between serum uric acid levels and BMI/dyslipidaemia. It was also observed that the uric acid levels increase with a longer duration of diabetes and are significantly higher in patients with cardiovascular complications like acute coronary syndrome, CCF, hypertension and arrhythmias. Finally, we can conclude that serum uric acid level above 5 mg/dL in diabetic patients is a marker or risk factor for cardiovascular complications.
Declaration of Conflicting Interest
The authors declare no conflict of interest.
Funding
This research received no external funding.
Ethical approval
The study protocol was reviewed and approved by the institutional research ethics committee of JJM Medical College, Davangere, Karnataka, India. Ethical approval no.- JJMMC/IEC/Sy-41-2016.
References
- Oberoi S, Kansra P. Economic menace of diabetes in India: a systematic review. Int J Diabetes Dev Ctries. 2020; 17:1-12.
- Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, Unwin N, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. 2019; 157:107843.
- IDF Diabetes Atlas 7th edition 2015.
- IDF Diabetes Atlas 6th edition; 34-68.
- Pan XR, Li GW, Hu YH, Wang JX, Yang WY, An ZX, et al. Effect of diet and exercise in preventing NIDDM in population with impaired glucose tolerance: the da qing IGT and diabetes study. Diabetic Care. 1997; 20:537-44.
- Ramachandran A, Jali MV, Mohan V, Snehalatha C, Viswanathan M. High prevalence of diabetes in an urban population in south India. BMJ. 1988; 297:587-90.
- Diabetes Prevention Program Research Group. Within-trial cost-effectiveness of lifestyle intervention or metformin for the primary prevention of type 2 diabetes. Diabetes Care. 2003; 26:2518-523.
- American Diabetes Association. Diagnosis and Classification of Diabetes Mellitus. Diabetes Care. 2006; 29:s43-s48.
- Chaturvedi N, Fuller JH, Taskinen MR, EURODIAB PCS Group. Differing associations of lipid and lipoprotein disturbances with the macrovascular and microvascular complications of type 1 diabetes. Diabetes Care. 2001; 24 (12):2071-077.
- Mustafa F. To Treat or Not to Treat Asymptomatic Hyperuricemia. Saudi J Med Med Sci. 2014; 2:95-100.
- Conen D, Wietlisbach V, Bovet P, Shamlaye C, Riesen W, et al. Prevalence of hyperuricemia and relation of serum uric acid with cardiovascular risk factors in a developing country. BMC Public Health. 2004; 4:9.
- Waring WS, Webb DJ, Maxwell SR. Uric acid as a risk factor for cardiovascular disease. QJM. 2000; 93(11):707-13.
- Pasalic D, Marinkovic N, Feher-Turkovic L. Uric acid as one of the important factors in multifactorial disorders – facts and controversies. Biochem Med (Zagreb). 2012; 22(1):63-75.
- Feig DI, Kang D-H, Johnson RJ. Uric acid and cardiovascular risk. N Engl J Med. 2008; 359(17):1811-821.
- Chen L-Y, Zhu W-H, Chen Z-W, Dai H-L, Ren J-J, et al. Relationship between hyperuricemia and metabolic syndrome. J Zhe-jiang Univ Sci B. 2007; 8(8):593-98 .
- Mishra US, Patra J. Study of serum uric acid level in diabetes mellitus with special reference to cardiovascular risk factors.J Evid Based Med Healthc. 2018; 5(9):753-61.
- Feig DI, Johnson RJ. Hyperuricemia in childhood primary hypertension. Hypertension. 2003; 42:247-52.
- Cannon PJ, Stason WB, Demartini FE, Sommers SC, Laragh JH. Hyperuricemia in primary and renal hypertension. N Engl JMed. 1966; 275(9):457-64.
- Lin K-C, Tsao H-M, Chen C-H, Chou P. Hypertension was the major risk factor leading to development of cardiovascular dis-eases among men with hyperuricemia. J Rheumatol. 2004; 31(6):1152-158.
- Johnson RJ, Kang D-H, Feig D, Kivlighn S, Kanellis J, Watanabe S, et al. Is there a pathogenetic role for uric acid in hyperten-sion and cardiovascular and renal disease? Hypertension. 2003; 41(6):1183-190.
- Ethmouda F, Elbrasai H, Elneihoum AM. Uric acid in chronic heart failure; correlation with prognostic markers. Ibonasina J Med BS. 2014; 6(5):208-12.
- Das A, Dhandapani E, Sugumar A, Manam A. Study of serum uric acid levels in acute myocardial infarction. Int J Pharm Bio Sci. 2015; 6(4):222-26.
- Martínez-Quintana E, Tugores A, Rodríguez-González F. Serum uric acid levels and cardiovascular disease: the Gordian knot. J Thorac Dis. 2016; 8(11):E1462-E1466.